

Why doesn't our immune system constantly attack our own bodies?
Peripheral Immune Tolerance - Nobel Prize 2025

A few months ago the Nobel Assembly at Karoliska Institutet announced the recipients of the Nobel Prize in Medicine/Physiology, having been awarded jointly to Mary E. Brunkow, Fred Ramsdell, and Shimon Sakaguchi for their groundbreaking discoveries concerning peripheral immune tolerance. This was in recognition of identifying the immune system’s security guards, known as the Regulatory T-Cells(or Treg Cells), and key Foxp3 gene that regulates these cells.

What are T-cells
T cells, or T lymphocytes, are a critical type of white blood cell that serves as the main fighting force of the body’s adaptive immune system. They are one of 2 primary cells responsible for the adaptive immune response(the other being B-cells). They identify pathogenic or infected cells using T-cell Receptors(TCRs) present on the the cell surface, which recognises pathogenic antigens presented by antigen presenting cells(i.e dendritic cells, macrophages etc).
This activates the T-cells, causing them to rapidly divide into 4 types of T-cells, CD4+ helper cells, CD8+ cytotoxic cells, Memory T-cells and the newly2 discovered CD25 T-Regulatory cells. T-regulatory cells inhibit the immune response once the threat is gone, preventing the immune system from attacking the body’s own tissues.
These are the functions of the different types of T-cells:
CD4+ Helper Cells: Enhance the immune response by activating B cells,
macrophages, neutrophils, eosinophils, and other immune cells, using specific cytokines/chemical signals
CD8+ Cytotoxic Cells: Kill infected or cancerous cells by inducing apoptosis(programmed cell death.
Memory Cells: These cells maintain “immunity” against the pathogen, allowing for the immune system to activate more efficiently upon exposure to the same pathogen again
CD4+CD25+ Regulatory T-Cells: They slow down or stop the immune response once the threat is gone, preventing the system from attacking the body’s own healthy tissues. These are the focus of this article and the nobel prize.
T-cells work together with B-cells to make up the adaptive immune response of the human body, with T-cells being in charge of cell-mediated response, which B-cells are in charge of humoral/antibody response.
.")
What is immune tolerance
Immune tolerance refers to the body’s ability to weed out immune cells that damage normal human cells, i.e autoimmune cells. This in T-cells is broken down into 2 areas: Central Immune Tolerance and Peripheral Immune Tolerance.
Central Immune Tolerance
The process of central immune tolerance takes place in the thymus, where immature t-cells[thymocytes] migrate to from the bone marrow and are fully developed.
Here they under go VDJ recombination, where unique T-cell Receptors[TCRs] are made from the random combination of different gene segments[VDJ], to produce unique T-cell surface receptors that will be able to bind to any pathogen that humans have or will come across. But this risks the developement of autoimmunity, where the TCR bind to antigen[cell identification markers] of their own body, i.e auto-immunity.
This is where the 3 selection checkpoints come in:
β-selection: Checks if the developing thymocytes are able to successfully form a functional pre-TCR
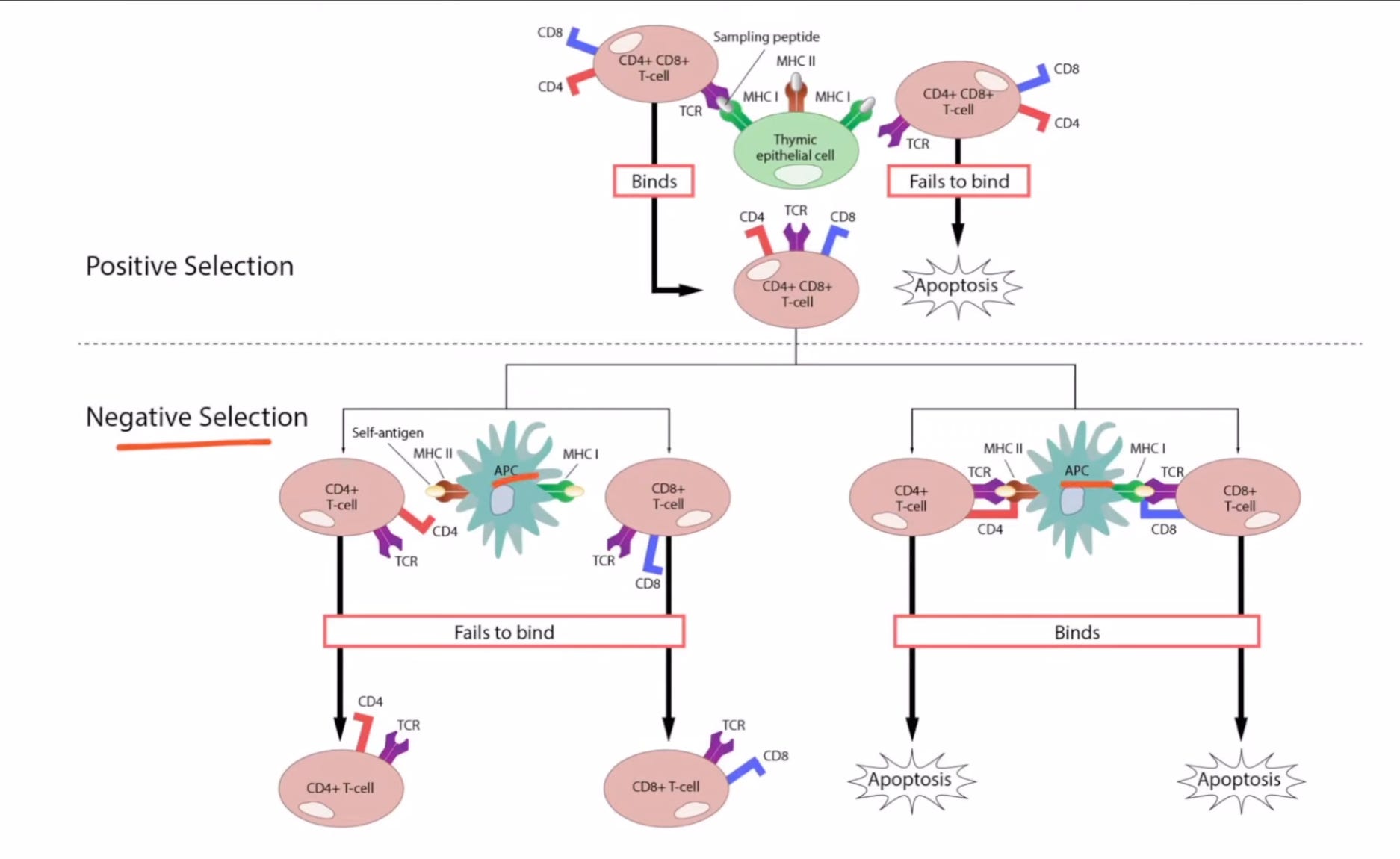
Positive Selection[MHC-recognition]: Checks if the TCR of the thymocytes are able to bind to either a MHC1 or MHC2 receptor. If it binds to a MHC1 receptor it becomes a CD4+ Helper T- Cell, while if it binds to a MHC2 receptor, it becomes a CD8+ Cytotoxic T-Cell.
Negative Selection[Central Tolerance]: Checks for T-cells that bind to self-antigens[human body antigens]. These cells then undergo apoptosis[programmed cell death] or become T-reg cells, depending on how strongly the bind to self-antigens.4
How were Regulatory T-cells discovered
Regulatory T-cells were originally identified in the 1972 under the name of “Supressor T-cells”, through the testing of the antigen-induced DNA synthetic response of different thymocyte populations. The main discovery from this experiment was that T-cells were capable to suppressing other types of T-cells. Before this it was widely believed that the only way to inhibit an immune response was through anti-bodies(made by B-cells), creating a feedback loop. 5 Before this, the importance of thymus-derived cells in preventing autoimmunity was demonstrated in 1969, through experiementation involving thymectomy & thymus transplantation in newborn mice.6 With these experiments, a new level of immune regulation, known as ‘peripheral tolerance’, was discovered, but speciifc markers & genes associated with this were still not identified.
That changed in 1995, when a team of scientists led by Dr Simon Sakaguchi(one of the Nobel Laureates) identified the CD25 antigen as being expressed by T-reg cells. This was done by depleting adult mice of CD25+CD4+ T-cells, which led to them developing auto-immune disorders evident at the histological and serological level. Putting them back after a while was able to prevent these problems in a dose-dependant fashion. These mice when exposed to external proteins shows heightened immune response after the removal of CD25+CD4+ cells, and adding them back returned the response back to normal. These 2 obervations thus proved that CD25+CD4+ cells contributed to auto-immune disease prevention and self-tolerance, by reducing immune response against self-antigens & external antigens. “Abnormality of this T cell-mediated mechanism of peripheral tolerance can be a possible cause of various autoimmune diseases.” 7
After this, in 2000, a group at Oxford discovered how T-reg cells work in vivo[in the body]. It was revealed that the immune-suppressive function of these cells was through the signaling of the CTLA-4 antigen & the secretion of a chemical known as immune-suppressive cytokine growth factor beta. CTLA-4, while it can be found on other immune cells, is continuously expressed on T-reg cells, indicating the possibility that T-reg function contributes to the immune-suppression of CTLA-4. 8
Based on this, in 2001, Dr Mary Brunkow & Dr Fred Ramsdell[the other 2 Nobel Laureates], identified the FOXP3 and linked mutation in the gene[its mouse counterpart Foxp3] to a fatal autoimmune disease in mice. It was found that the mutation in it preventing the production of functional T-reg cells. The gene was then linked to a IPEX syndrome, a fatal congenital autoimmune disease. 910 Today its been recognised that the FOXP3 gene makes the critical FOXP3 protein which is the key transcriptional factor for T-reg Cells. 11

Applications in Modern Medicine
Cancer
CCL5, a chemical cytokine that has a major role in regulating immune responses, is highly expressed in tumour tissue. CCL5 recruits T-reg cells into the tumour and secretes TGF-β, suggesting that the number & immuno-suppressive function of T-reg cells increases in cancer patients. Furthermore, it has been found that other biomarkers such as PD-L1 & CTLA-4 are highly expressed on the surface of T-reg cells. All this suggests that T-reg cells may aid in tumour progression.
In labs with single-cell sequencing technique, it has been found that certain T-reg cell types can worsen tumour effects. For example, higher percentages of Helios+CCR8+ Treg cells are associated with a poorer pancreatic cancer prognosis.
CTLA-4, as mentioned earlier, is a key antigen/bio-marker for T-reg cells. Thus deleting is in T-reg cells leads to tumour immunity, and anti-CTLA-4 antibodies have been shown to cause a reduction in T-reg cells and improve immune action against tumour cells11
Neurodegenerative Disorder
Alzheimers(AD) and Parkinson’s Disease(PD) are caused by chronic oxidative stress and inflammatory dysregulation. Patients with AD and PD show increased frequency and enhanced suppressive activity of activated T-reg cells. Tregs protect neurons from inflammatory damage and help maintain the balance between Th17[a pro-inflammatory subtype of the CD4 Helper Cell] and T-reg cells.
There is however, a new “Baruch Finding”, where temporary depletion of T-reg cells can actually help the brain’s choroid plexus recruit more immune cells to clear amyloid-β plaques and mitigate inflammation.11
Cardiavascular Disease
Artherosclerosis is the primary cause of most Cardiovascular disease. It is causes by blood vessel wall damage, causing inflammation, leading to plaque build-up. Increasing T-reg cells in the aorta and lymph nodes can reduce T-cell activation, reducing inflammation and thus slowing the disease. In atherosclerosis and ischemic cardiomyopathy, T-reg cells can lose their protective nature, becoming pro-inflammatory.
That said, similar to the “Baruch Finding”, in mouse models of cardiomyopathy[heart muscle disease], periodic depletion of T-reg cells has been shown to reverse heart failure.11
Metabolic Diseases - Diabetes
Type 2 Diabetes(T2D): Patients have shown a decrease in the ratio of T-reg cells to CD4 cells[specifically Th1 & Th17 sub-types]. Specifically, a reduction in CD39+ Treg cells is linked to an inability to suppress harmful Th17 cells.
Type 1 Diabetes(T1D): Due to the autoimmune nature of T1D, transferring autologus T-reg cells back into patients has been used to protect insulin-producing β-cells.
Age-Related Insulin Resistance: Contrary to their effects above, T-reg cells accumulate in adipose(fat) tissue in mice models of older/obese mice, leading to insulin sensitivity. 11
Muscle Atrophy
T-reg cells are important for skeletal. muscle repair, and accumulate in injury sites ~4 days after damage. They secrete Aphiregulin(Areg), which directly promotes regeneration of muscle stem cells. The exact mechanism of this is still being research. 11
T-reg cell therapies
These are being developed as tools to treat autoimmune and inflammatory disease, preventing graft-versus-host disease (GvHD), and promoting organ transplant tolerance. This is being done with a similar technology to CAR-T cell therapies that are being rolled out. 12

And thats it for this one.
https://www.akadeum.com/t-cell/
by newly it means 1992, but considering most that T cells were originally discovered in the 1960s, with CD4+ Helper & CD8+ Cytotoxic T-cells being identified in 1968 & 1970 respectively. Only T-memory cells came after in the late 1990s
https://myhematology.com/white-blood-cells/t-cell-acute-lymphoblastic-leukemia-t-all/
https://academic.oup.com/jimmunol/article-abstract/108/3/586/8094028?redirectedFrom=fulltext
https://pubmed.ncbi.nlm.nih.gov/5823314/
https://pubmed.ncbi.nlm.nih.gov/7636184/
https://pubmed.ncbi.nlm.nih.gov/10899916/
https://pubmed.ncbi.nlm.nih.gov/11685453/
https://pubmed.ncbi.nlm.nih.gov/11137993/
https://pubmed.ncbi.nlm.nih.gov/33529458/
https://pmc.ncbi.nlm.nih.gov/articles/PMC12615433/#s4